
In late June Bike Ottawa submitted a letter regarding the plans for the New Civic Hospital, providing an overview of our concerns, and what it means for sustainable and active transportation in and around the proposed hospital campus. At the time we promised to return with a more granular look at the massive document.
The following is the first of two blog postings showcasing our more fine detail look at the proposed hospital plans.
We have broken down our examination of the hospital plan into 4 sections: Modal Share, Transportation Demand Management (TDM), Infrastructure and Parking.
In today’s post you can read our thoughts on modal share and the TDM. In short, the modal share, which is the foundation for the entire site plan, is based on a poorly thought out evaluation of modal share and the shifting goals of the City of Ottawa in the New Official Plan (OP). The new OP calls for the majority of trips to be made by sustainable transportation in Ottawa. The plans for the new hospital, however, do not reflect this, and while the hospital plan proposal comes just before the new OP is approved, the repercussions of the new hospital plan will last well into the future, and we believe the hospital plans should reflect the new OP goals and mandates, not the old ones.
The TDM we’ll give that a passing grade, and say it’s a good plan with many good elements, but there is no accountability in it. How does the hospital plan on implementing it? Who are they accountable to? How can the public and the residents trust they will implement what they are suggesting?
Below is our cover letter, followed by the Modal Share and TDM feedback:
To: Sean Moore, Planning, Infrastructure and Economic Development Department, City
of Ottawa
CC: Councillor Glen Gower, Co-Chair, Planning Committee
Councillor Scott Moffatt, Co-Chair, Planning Committee
Councillor Laura Dudas, Member, Planning Committee
Councillor Tim Tierney, Member, Planning Committee
Councillor Jeff Leiper, Member, Planning Committee
Councillor Riley Brockington, Member, Planning Committee
Councillor Allan Hubley, Member, Planning Committee
Councillor Catherine Kitts, Member, Planning Committee
Councillor Jenna Sudds, Member, Planning Committee
Councillor Jean Cloutier, Member, Planning Committee
Councillor Shawn Menard, Member, Planning Committee
Mayor Jim Watson
Councillor Catherine McKenney, Somerset Ward
Via email: TOH@ottawa.ca, glen.gower@ottawa.ca, Scott.Moffatt@ottawa.ca,
laura.dudas@ottawa.ca, tim.tierney@ottawa.ca, Jeff.Leiper@ottawa.ca,
riley.brockington@ottawa.ca, Allan.Hubley@ottawa.ca, Catherine.Kitts@ottawa.ca,
Jenna.Sudds@ottawa.ca, Jean.Cloutier@ottawa.ca, capitalward@ottawa.ca,
Jim.Watson@ottawa.ca, Catherine.Mckenney@ottawa.ca,
Date: August 19, 2021
Subject: Ottawa Hospital New Civic Campus Transportation Plan
Dear Mr. Moore,
Bike Ottawa is a non-profit, volunteer-based organization that advocates for safe bike infrastructure in Ottawa. This letter provides feedback on the transportation study for the proposed new Civic Hospital campus and follows up on a letter that we sent on June 18, 2021 with high-level feedback on the study.
In light of the scope of the new Civic Hospital campus—its size, the funding it will require, the lives it will affect, and its lifespan—we believe this project should be afforded careful consideration. This scope also means there are many opportunities to do much good, but equally many for detrimental consequences. In this letter, we have identified a number of laudable parts of this plan, as well as many that fall short of the high aspirations that a project of this scope ought to have. In order to render our feedback clear and digestible, we have organized our recommendations into four separate documents; they address:
- projected modal shares
- infrastructure
- bike parking
- the Transportation Demand Management plan
Please note that all page references in our feedback refer to the first draft of the transportation study, not the revised version issued on July 30, unless otherwise specified.
We thank you in advance for your consideration of our concerns. Please feel free to
contact us, should you have any questions. Bike Ottawa would be happy to work with
you on any details of this project.
Sincerely,
Bike Ottawa
Érinn Cunningham, President
Barbara Greenberg, Board Member
Dave Robertson, Board Member
William van Geest, Chair, Advocacy Working Group
Christie Cole, Chair, Equity Committee
John Black, Member, Advocacy Working Group
New Civic Hospital Campus Transportation Study: Modal shares
This document concerns projected modal shares at the new campus of the Ottawa Civic Hospital (TOH) as they arise in the Transportation Impact Assessment and Mobility Study (TIA). We devote an entire document to modal shares for two reasons. First, modal-share estimates play an important role in the infrastructure planned for the site; where these estimates are incorrect, planned infrastructure will end up being inadequate. Second, modal-share estimates reflect the priorities of planners for a given site; in the present case, Bike Ottawa believes that the TOH priorities for the new Civic hospital are inappropriate, as we will show.
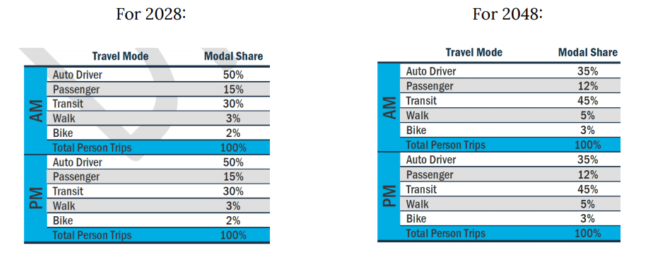
The modal-share projections in the TIA are as follows (pp. 33–34):
The TIA also envisions a “worst-case scenario,” wherein in 2028, 65% of people accessing the site would access the site by driving a car there—that is, 15 percentage points more than hoped (pp. 32, 34):
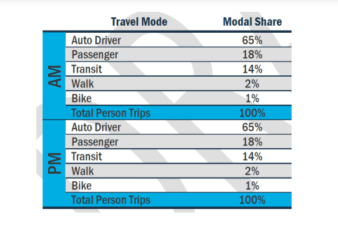
We note that for 2028, the modal shares are 3% for walking and 2% for biking; and for 2048, 5% for walking and 3% for biking—or, in the “worst-case scenario” for 2028, 2% for walking and 1% for biking.
We are encouraged that in many places, the TIA acknowledges the importance of promoting sustainable transportation—not only for the health and well-being of those accessing the hospital, nor yet to properly integrate with the City of Ottawa, but also for the basic functioning of the institution. We are concerned, however, that the TIA’s plans do not reflect these realities. Our main concerns are the following:
- the transportation study is oriented toward maintaining a status quo, not to promoting sustainable, efficient transportation habits
- the modal shares are based on unrepresentative numbers
- those numbers are already low because of poor transportation policies and infrastructure at the existing Civic Hospital campus
- the TIA’s consideration of transportation patterns at peer institutions is good, but the conclusions drawn from these considerations are unhelpful
- as a tool for projecting traffic patterns, ITE trip generation is automobile-centric, and so it is no surprise that the recommendations it yields are themselves automobile-centric
The TIA clearly acknowledges the importance of promoting non–private vehicle modes of transportation for the very functioning of the hospital. For example, the TIA acknowledges that “Reducing the number [of] trips by personal vehicle will be critical to maintain reasonable operation of the adjacent [to the site] road network” (p. 70).
Further, “TOH should endeavor to reduce personal vehicle use by staff and visitors as much as possible” to avoid exceeding car-parking supply (p. 70). In fact, the TIA calls the need for a proactive approach to managing transportation impacts “essential” (p. 70) and signals the possible need for “more aggressive non-auto mode share targets” (p. 52).
But the TIA’s concrete plans do not reflect these observations. The closest that the TIA’s plans come is in the Transportation Demand Management plan (TDM); but, as our analysis of the TDM (enclosed) shows, the TDM remains too speculative and non-committal at this stage.
Modal-Share Estimates
An important problem with the TIA’s modal-share targets for the new Civic Hospital campus is how these targets relate to modal share estimates at the existing Civic Hospital campus, which are effectively 0% for both biking and walking (p. 28). As a basis for these estimates, the plan cites “discussions with TOH staff,” providing no further specifications as to either the nature of these discussions or which TOH staff were involved. We fear these discussions were informal and involved minimal research, if any. Regardless of its nature, any research on this topic should be detailed in the TIA. By comparison, estimates for current car travel to the existing Civic Hospital campus fill many pages of the TIA. (We are also concerned by underdeveloped methodologies in other parts of the TIA; for example, the TIA also cites “discussions with TOH staff” for the opinion that car parking at the existing campus “exceed[s] the available parking supply” (p. 61), as well as a vague reference “field collection by Parsons staff” (p. 15).)
Based on these unspecified “discussions,” the TIA estimates modal shares for walking and biking at the existing Civic Campus to be “negligible,” and proceeds to omit walking and biking from further consideration of current modal shares; that is, their share is calculated as 0%. Yet the evidence at the campus tells another story: an informal survey of bikes parked at the existing Civic campus during a weekday in June 2021 yields approximately 100 bikes. This suggests that at least 100 people bike to the campus on a typical day. Since the TIA does not include final figures on person trips to the existing Civic Hospital campus, we cannot calculate what proportion of modal share this represents, but we estimate this to be in the range of 2–3%. Since we do not have data on walking trips to the existing Civic Hospital campus, moreover, we cannot provide an estimate of this modal share.
Finally, TIA also relies for its modal-share estimates on “comprehensive surveys in 2011 on travel behaviour in the National Capital Region” (p. 29). Yet the City of Ottawa’s bike network has improved considerably in the last ten years, and data from 2011 will of course not reflect these improvements. In light of the above, Bike Ottawa is concerned that TOH’s estimates of modal shares for biking and walking at the existing Civic Hospital campus are inaccurate—in part because they are also under-examined. Because these estimates are an important basis for TOH’s projections for walking and biking for the new Civic Hospital campus, these projections are flawed from the start.
Modal-Share Projections
Bike Ottawa also believes that the modal-share projections for biking and walking at the new Civic Hospital campus are too low. To begin with, these projections are low relative to the opportunities the proposed site affords. The TIA itself acknowledges that the new campus will be much better connected than the current campus; it calls this campus “centrally located” (p. 5). On one hand, it promises “far superior pedestrian and cyclist infrastructure than the existing Civic Campus” (p. 52); on the other hand, it acknowledges that it “will be located in a significantly better transit catchment area, directly adjacent to the Dow’s Lake LRT Station and the aforementioned Carling Avenue Transit Priority Corridor” (p. 52). In light of this good connectivity, one would expect much better modal shares for non-automobile travel.
The modal shares for biking and walking are also low relative to the study of comparable institutions discussed in the TIA . This study included other institutions in Ottawa, several Toronto hospitals, and some hospitals in the United States (pp. 29–33). The TIA identifies two institutions as particularly good fits for comparisons of modal shares with the new Civic campus: Carleton University and Toronto Western Hospital (see table).
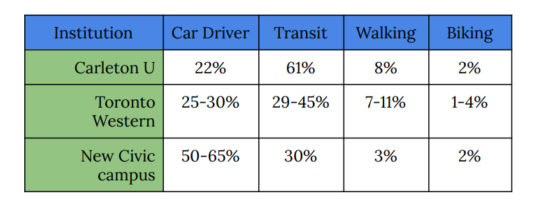
Yet in setting its own modal-share targets, the TIA ultimately seems to ignore these institutions: its projections at the new Civic campus for automobile use, for example, are at least double those of either institution. This disparity is particularly perplexing given that the shares for other institutions are for current patterns, and those for the new Civic campus are for 2028—almost ten years later.
The projected modal shares are low even relative to the City of Ottawa’s own official documents. City of Ottawa’s Transportation Master Plan (2013) sets targets of 10% for walking and 5% for biking by 2031 (p. 23). These goals will not even be met in the projections for 2048 for the new Civic campus, which project a 5% share for walking and a 3% share for biking (p. 33). In sum, we find this plan wholly lacking in aspiration with respect to its modal-share projections.
Finally, one of the tools that the TIA uses to generate its modal-share projections, ITE trip generation rates—is inappropriate. The TIA even acknowledges the major shortcomings of this approach (p. 26):
- The majority of ITE studies only recorded vehicle trips and do not provide mode share statistics for the surveyed site. Therefore, assumptions have to be made to estimate person-trips, which increases the margin for error.
- ITE surveys were mainly conducted in the United States, which has a significant number of private hospitals that tend to be smaller in size compared to public hospitals in Canada.
- ITE surveys were completed in the 1980s, 90s and early 2000s. Transportation systems have evolved significantly in Canada over the last three decades. By the TIA’s own admissions, then, ITE trip generation rates are inappropriate for projecting modal shares for the new Civic campus.
Conclusion
In sum, Bike Ottawa believes that the modal-share projections in the TIA are poorly founded and warrant revision. We believe the basis for these projections, estimates of modal shares at the current Civic Hospital campus as well as ITE trip-generation rates, are problematic. We note that while the TIA itself outlines several ways in which modal shares for biking and walking could be much higher than they currently are, as well as the importance that they be so, its projections fail to reflect this. As a minimum, these projections should keep step with the City of Ottawa’s official documents. Better would be if they reflected what the TIA shows is possible at comparable institutions. Best, however, would be if TOH set targets that reflected some aspiration and ensured the best functioning of the new Civic Hospital campus—high shares for efficient modes like public transit, walking, and biking—and then build infrastructure to accommodate these modes.
Bike Ottawa thanks TOH in advance for its consideration of our feedback concerning modal shares for the new Civic hospital campus. We invite TOH to contact us if it has any questions about our feedback. We would also be glad to work with TOH on these and any other measures and policies.
New Civic Hospital Campus Transportation Study: Transportation demand management
This document concerns the Transportation Demand Management plan (TDM) presented in the Transportation Impact Assessment and Mobility Study (TIA) for the new campus of the Ottawa Civic Hospital (TOH).
Bike Ottawa was pleased to see the inclusion of a TDM in the TIA. In fact, we believe that the TDM is one of the stronger parts of the TIA—at least, in its acknowledgement of the importance of proper support for biking, walking, and public transit at the new Civic campus. As the TIA states, “it is expected that more aggressive mode share targets for alternate modes (e.g. transit, walking and cycling) will be required” for the hospital to function smoothly, and this “requires the implementation of a robust and comprehensive Transportation Demand Management (TDM) Plan to increase the probability of success” (p. 65). The TDM also correctly acknowledges that “Reducing the number trips by personal vehicle will be critical to maintain reasonable operation of the adjacent road network” (p. 70). We were also pleased to see the TIA’s interest to this end—“to increase sustainable modes and reduce dependency on the personal vehicle” (p. 71).
We were also glad to see examples in the plan from other comparable North American institutions of policies and measures that would help achieve these goals. For example, the Seattle Children Hospital’s policies produced a reduction of 500 car-parking spaces in an institution with less than one-third the number of employees at this campus (pp. 71–72). We believe that by properly implementing a TDM, the new Civic campus can also drastically reduce the number of trips to the campus taken by car.
Apart from finer-grained recommendations, we have two general concerns. First, we are concerned about accountability: by what mechanism will the principles outlined in the TDM be applied? What powers will the “coordinator” mentioned in the TDM have to apply the TDM’s provisions? The TIA contains no details to this effect. Second, we are concerned that the proposed measures and policies remain too speculative and vague. This is reflected in TDM’s language: for example, it refers to measures and policies “that should be considered” (p. 72), and many of the items in the TDM checklists (Appendix S), while marked “highly recommended,” also indicate that they will be considered at an unspecified later stage. This approach toward the TDM is incommensurate with its importance to the hospital’s function, which the TIA itself acknowledges.
Bike Ottawa supports the following policies and measures:
- the establishment of a full-time equivalent (FTE) staff position for a TDM coordinator along with a TDM specific capital budget, as well as regular monitoring of travel-related behaviours and attitudes to better meet sustainable transportation goals
- consideration of financial incentives for sustainable modes; particularly those for active transportation will pay dividends in terms of long-term health benefits and general quality of life
- the creation of regular educational and promotional programs for employees, to make them aware of the benefits of active transportation and equip them with the knowledge to do so (to this end, we would recommend coordination with the EnviroCentre, who has experience with such programs)
- the creation of an emergency ride home program (ERH)
- acknowledgement of the importance of secure, well-located bike-parking space in ample supply, as well as an additional “buffer” of increased capacity—although these numbers will need to be adjusted for better modal-share projections (we discuss both bike parking and modal-share projections in separate documents in the present letter)
- the provision of showers, lockers, and change rooms
- the provision of adequate wayfinding signage (although this should include bike parking, which the TDM does not mention)
- the provision of trip-planning tools like mobile applications
We do have concerns about some aspects of the TDM, however:
- we are unclear why “on-site cycling courses for commuters, or subsidize off-site courses” is listed as “not appropriate,” when the TIA also acknowledges this measure as “one of the most dependably effective tools to encourage the use of sustainable modes” (Appendix S, p. 10)
- we are disappointed that two key measures are listed as “Opportunity limited due to site constraints”: 1) “Locate building close to the street, and do not locate parking areas between the street and building entrances,” and 2) “Locate building entrances in order to minimize walking distances to sidewalks and transit stops/stations” (Appendix S, p. 5). The “site constraint” in question appears to be the positioning of the largest parking structure between the Dow’s Lake LRT station and the hospital’s main entrance. The TIA rightly lists these measures in first and second place, but the plan does not meet the standard it sets out
- while we support the idea of including on-site bikeshare stations and the provision of bike-share memberships to employees, we note that no bike-share program currently exists in Ottawa. We suggest that TOH work with the City of Ottawa to develop a bike-share program, in light of its obvious value
- we recommend that TOH initiate a bike loan program for employees to provide them a low-risk opportunity to transition to commuting by bike
- we recommend that TOH initiate a program whereby long-term patients may be taken out for bike rides. Biking has a low physical impact yet affords people the opportunity to exercise and/or travel efficiently; indeed, bikes are for many people accessibility devices. Programs like Cycling Without Age have bikes that may be able to take long-term patients out for rides.
Bike Ottawa thanks TOH in advance for its consideration of our feedback concerning
the TDM for the new Civic hospital campus. We invite TOH to contact us if it has any
questions about our feedback. We would also be glad to work with TOH on these and
any other measures and policies.